
FAQ – Frequently asked questions

What is a pessary?
Vaginal support pessaries support the bladder, urethra and/or uterus from the vagina. They are mainly made of injection moulded silicone.
For decades different types of pessaries, especially cube, sieve cup, ring and urethra pessaries, have proven to be a non-surgical method of treatment for gynaecological clinical syndromes, such as descensus and its symptoms and stress urinary incontinence.
What material is restifem made of and what is its compatibility?
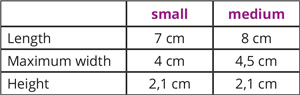
What restifem sizes are available and what are the product dimensions?
How do I choose the right size for me?
In principle, you can test yourself which pessary size is the correct one. No pain should be felt when wearing the pessary and no contact bleeding should occur. However, an initial feeling of pressure towards the uterus and behind the pubic bone is desirable, as the tissue structures in these areas should be relieved, i.e. supported.
If you are not sure which is the right size, either choose the set or consult your attending gynaecologist.
When can I start pessary therapy after the birth of my child?
Can my treating doctor prescribe restifem by prescription?
Other countries have different regulations. Please consult your attending physician or your health insurance company for more information.
Where can I buy restifem?
Can I get a retroactive discount if I buy the two sizes separately instead of the set in advance (116 Euros versus 98 Euros)?
Can I cancel the purchase of restifem after opening the foil bag?
As a physiotherapist, can I order a restifem sample from you?
How can the preventive effect of restifem be explained?
The way restifem works can be explained as follows: If you sprain your ankle, you will feel pain and instability while running. A support bandage provides immediate stability, relieves pain and supports the regeneration of the retaining ligaments and joint capsule. A postnatal pessary therapy has a comparable effect. For example, the pessary pushes the uterus into the initial position, as it was before the pregnancy. The posterior ligament of the uterus is thus relieved and can regenerate optimally. In contrast to some other pessaries, restifem does not put additional strain on the pelvic floor muscles due to its retropubic support mechanism.
However, the preventive effect of postpartum pessary therapy over the course of a lifetime is scientifically difficult to demonstrate, because many factors contribute to the development of a descensus or urinary incontinence and the first symptoms often occur only after years or even decades. Above all, these factors are number of pregnancies, vaginal births, gynaecological operations, ageing processes (especially due to the hormonal changes in the menopause) but also obesity, lack of exercise, and heavy physical work.
How can I additionally support the natural recovery processes, especially the recovery of the pelvic floor connective tissue, after a birth?
The following therapeutic approaches are available to support the recovery of the pelvic floor connective tissue (source: Beilecke (2019) Postpartum influence on the pelvic floor connective tissue – a therapeutic approach that has been neglected up to now. Gynaecologist: 505-507):
1. Pessary therapy e.g. restifem
2. Local oestrogen therapy – oestrogen promotes wound healing in the pelvic floor connective tissue by activating fibroblasts and thus the formation of new connective tissue. A doctor can prescribe vaginal hormone therapy with Estriol, provided there are no medical contraindications.
3. Neural therapy – injection with local anaesthetics helps to improve wound healing and relieve pain.
4. Vitamin D substitution – vitamin D has an anti-inflammatory and immunomodulating effect via its hormone. There is a correlation between the level of vitamin D and the strength of the pelvic floor muscles. In the systemic substitution of vitamin D from breastfeeding women, the transfer to the child must also be considered. The mother’s substitution should be carried out carefully and that of the child should be paused under certain circumstances.
5. Laser therapy – postnatal laser treatment promotes the regeneration of the connective tissue of the vaginal wall by activating fibroblasts and thus forming new connective tissue.
Can I wear restifem whilst doing pelvic floor exercises and other sports?
The pessary does not remain behind the pubic bone but is pushed towards the vaginal outlet. It almost slips out. Am I the wrong size or have I inserted it incorrectly?
The cause is usually a more pronounced state of descensus, which may have been caused, for example, by birth injuries (levator tearing, etc.). The abdominal pressure on the pessary is then so great that it cannot anchor behind the pubic bone and is pressed out of the vagina again.
Each descensus is highly individual in terms of type (uterus and/or vaginal walls) and severity (minor to complete prolapse). Please consult your treating physician regarding pessary therapy. If necessary, other pessary forms (e.g. a cube pessary) can give better hold.
After my pregnancy, I suffered from bladder prolapse and restifem was not sitting optimally. Now, after 15 weeks, my prolapse has improved and restifem has a better hold. What is the explanation for this?
Postnatal symptoms of descensus or prolapse are often spontaneously reduced due to the postnatal recovery processes in the connective tissue and the muscles of the pelvic floor. It is possible that restifem® will hold better after a few weeks and can support the natural recovery processes in a preventive way.
Moderately pronounced descensus/prolapse and urinary incontinence problems can be alleviated or eliminated by restifem.
restifem Service
balance

control

descensus-related problems

centre
